Now Reading: Understanding Urothelial Carcinoma: Causes, Symptoms, and Treatment
-
01
Understanding Urothelial Carcinoma: Causes, Symptoms, and Treatment
Understanding Urothelial Carcinoma: Causes, Symptoms, and Treatment
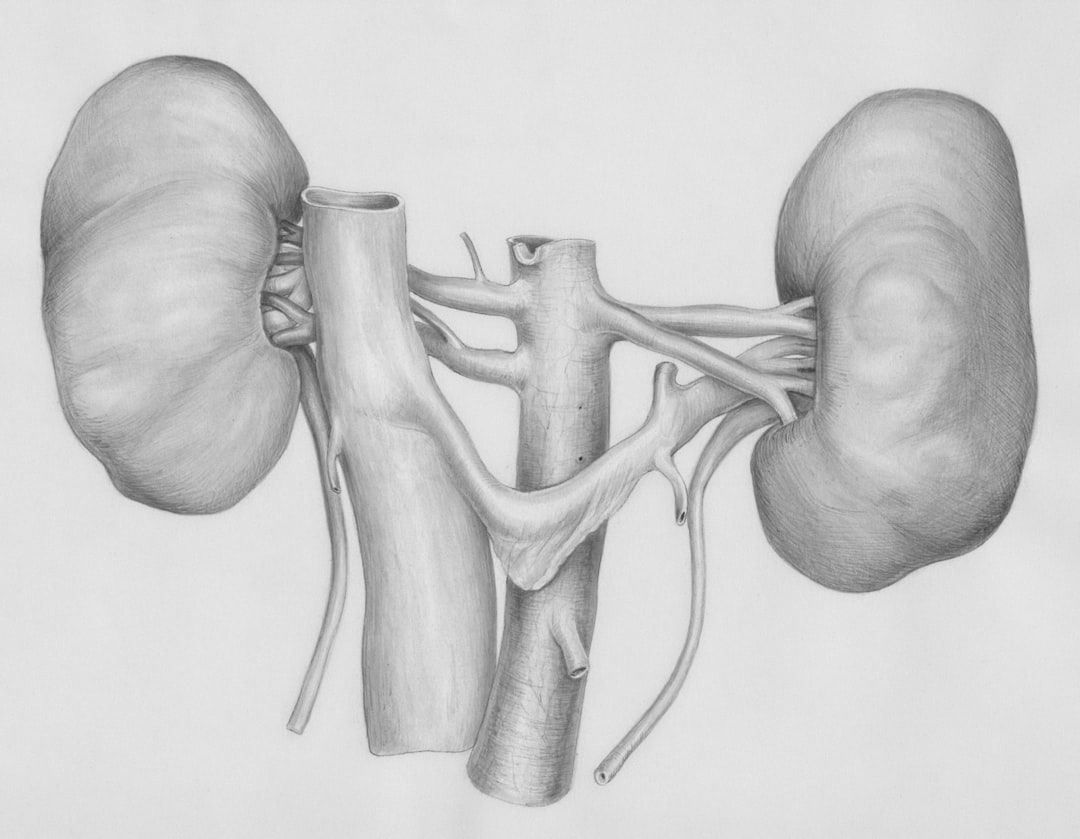
Urothelial carcinoma, also known as transitional cell carcinoma, is a malignancy that originates in the urothelium, the tissue lining the bladder, ureters, and part of the kidneys.
Urothelial carcinoma is the most prevalent form of bladder cancer, accounting for approximately 90% of all cases.
It can also occur in other parts of the urinary tract, making it a significant concern in urological oncology. The pathogenesis of urothelial carcinoma involves a complex interplay of genetic mutations and environmental factors. The disease can manifest in various forms, ranging from superficial tumors confined to the bladder lining to invasive forms that penetrate deeper into the bladder wall and beyond.
The World Health Organization classifies urothelial carcinoma into several grades and stages, which are crucial for determining prognosis and treatment strategies.
Key Takeaways
- Urothelial Carcinoma is a type of cancer that starts in the urothelial cells, which line the inside of the bladder, ureters, urethra, and renal pelvis.
- Risk factors for Urothelial Carcinoma include smoking, exposure to certain chemicals, chronic bladder inflammation, and genetic factors.
- Common symptoms of Urothelial Carcinoma include blood in the urine, frequent urination, pain during urination, and back or pelvic pain.
- Diagnostic tests for Urothelial Carcinoma include urine cytology, cystoscopy, biopsy, imaging tests, and molecular testing.
- Stages of Urothelial Carcinoma range from stage 0 (cancer is only in the innermost layer of the bladder) to stage IV (cancer has spread to nearby lymph nodes or other organs).
Risk Factors for Urothelial Carcinoma
Several risk factors have been identified that increase the likelihood of developing urothelial carcinoma. Smoking is one of the most significant contributors, with studies indicating that smokers are three to four times more likely to develop bladder cancer compared to non-smokers. The carcinogenic compounds in tobacco smoke can be excreted in urine, where they come into direct contact with the urothelium, leading to cellular damage and mutations.
Occupational exposure to certain chemicals is another notable risk factor. Individuals working in industries such as dye manufacturing, rubber production, and chemical processing may be exposed to aromatic amines and other carcinogens that have been linked to urothelial carcinoma. Additionally, chronic conditions such as urinary tract infections and bladder stones can contribute to the development of this malignancy by causing persistent irritation and inflammation of the bladder lining.
Common Symptoms of Urothelial Carcinoma
The clinical presentation of urothelial carcinoma can vary widely among patients, but several common symptoms are frequently reported. Hematuria, or blood in the urine, is often the first noticeable sign and can range from microscopic to gross hematuria. Patients may also experience dysuria, characterized by painful urination, and increased urinary frequency or urgency. In more advanced stages, patients may present with additional symptoms such as pelvic pain, weight loss, and fatigue. These systemic manifestations may indicate metastatic spread of the disease beyond the urinary tract. It is essential for individuals experiencing these symptoms to seek medical evaluation promptly, as early detection significantly improves treatment outcomes.
Diagnostic Tests for Urothelial Carcinoma
| Diagnostic Test | Sensitivity | Specificity | Accuracy |
|---|---|---|---|
| Urinalysis | 73% | 82% | 78% |
| Cystoscopy | 91% | 83% | 87% |
| CT Urography | 94% | 88% | 90% |
The diagnostic workup for urothelial carcinoma typically begins with a thorough medical history and physical examination. Urinalysis is often performed to detect hematuria or abnormal cells indicative of malignancy. If initial findings suggest cancer, further imaging studies such as ultrasound, computed tomography (CT) scans, or magnetic resonance imaging (MRI) may be utilized to assess the extent of disease and identify any potential metastases.
Cystoscopy is a critical diagnostic procedure that allows direct visualization of the bladder’s interior. During this procedure, a thin tube with a camera is inserted through the urethra into the bladder, enabling urologists to identify tumors and obtain biopsy samples for histopathological examination. The results from these tests are essential for confirming a diagnosis and determining the appropriate treatment plan.
Stages of Urothelial Carcinoma
Urothelial carcinoma is staged based on the extent of tumor invasion and spread. The American Joint Committee on Cancer (AJCC) staging system categorizes this malignancy into five stages: – Stage 0: Non-invasive papillary carcinoma or carcinoma in situ (CIS) confined to the urothelium.
– Stage I: Tumor invades the lamina propria but not the muscle layer.
– Stage II: Tumor invades the muscularis propria.
– Stage III: Tumor invades surrounding tissues or organs.
– Stage IV: Tumor has metastasized to distant lymph nodes or organs. Understanding the stage of urothelial carcinoma is crucial for determining prognosis and guiding treatment decisions.
Early-stage tumors generally have a better prognosis compared to those diagnosed at advanced stages.
Treatment Options for Urothelial Carcinoma
The treatment approach for urothelial carcinoma is multifaceted and depends on various factors including tumor stage, grade, patient health status, and preferences. Treatment modalities may include surgery, chemotherapy, immunotherapy, radiation therapy, and targeted therapy. A multidisciplinary team typically collaborates to develop an individualized treatment plan that optimally addresses each patient’s unique circumstances.
For superficial tumors (stages 0 and I), intravesical therapy with Bacillus Calmette-Guérin (BCG) or chemotherapy agents may be employed to reduce recurrence rates. In contrast, invasive tumors (stages II-IV) often necessitate more aggressive interventions such as radical cystectomy or systemic chemotherapy.
Surgery for Urothelial Carcinoma
Surgical intervention remains a cornerstone in the management of urothelial carcinoma, particularly for localized disease. Radical cystectomy involves the complete removal of the bladder along with surrounding tissues and lymph nodes. In men, this may also include prostatectomy, while in women, a hysterectomy may be performed.
For patients with non-muscle invasive disease, transurethral resection of bladder tumor (TURBT) is often utilized to excise visible tumors while preserving bladder function. Surgical options are tailored based on tumor characteristics and patient preferences regarding quality of life post-surgery.
Chemotherapy and Immunotherapy for Urothelial Carcinoma
Chemotherapy plays a pivotal role in treating advanced urothelial carcinoma. The most commonly used regimens include cisplatin-based combinations such as MVAC (methotrexate, vinblastine, doxorubicin, cisplatin) or gemcitabine plus cisplatin. These agents work by targeting rapidly dividing cancer cells but can also affect normal cells, leading to side effects such as nausea, fatigue, and immunosuppression.
Immunotherapy has emerged as a promising treatment modality for advanced urothelial carcinoma. Immune checkpoint inhibitors like pembrolizumab and atezolizumab have shown efficacy in patients with metastatic disease who have progressed after chemotherapy. These agents enhance the immune system’s ability to recognize and attack cancer cells by inhibiting proteins that suppress immune responses.
Radiation Therapy for Urothelial Carcinoma
Radiation therapy may be employed as an adjunctive treatment for urothelial carcinoma in specific scenarios. It can be utilized postoperatively to eliminate residual cancer cells following surgery or as a palliative measure to alleviate symptoms associated with advanced disease. External beam radiation therapy (EBRT) is commonly used in these cases.
While radiation therapy can be effective in controlling local disease progression, it is essential to consider potential side effects such as cystitis or damage to surrounding tissues. Therefore, careful planning and monitoring are crucial during treatment.
Targeted Therapy for Urothelial Carcinoma
Targeted therapy represents a novel approach in treating urothelial carcinoma by focusing on specific molecular targets associated with cancer growth and progression. Agents such as erdafitinib target fibroblast growth factor receptor (FGFR) mutations commonly found in bladder cancer patients. This therapy has shown promise in patients with advanced disease who harbor these genetic alterations.
The development of targeted therapies has revolutionized treatment paradigms by offering options that are often better tolerated than traditional chemotherapy while providing significant clinical benefits.
Prognosis and Survival Rates for Urothelial Carcinoma
The prognosis for patients diagnosed with urothelial carcinoma varies significantly based on several factors including tumor stage at diagnosis, histological grade, and response to treatment. According to recent statistics from the American Cancer Society, the five-year survival rate for localized bladder cancer (stages 0-I) is approximately 96%, while this rate drops to around 15% for metastatic disease (stage IV). Early detection through regular screening and prompt intervention remains critical in improving survival outcomes.
In summary, urothelial carcinoma is a prevalent malignancy affecting the urinary tract that necessitates a comprehensive understanding of its risk factors, symptoms, diagnostic methods, staging, and treatment options. With advancements in surgical techniques, chemotherapy regimens, immunotherapy approaches, radiation therapy modalities, and targeted therapies, there is an increasing potential for improved patient outcomes and survival rates.
Early detection remains paramount in enhancing prognosis and ensuring effective management strategies are implemented promptly.
If you or a loved one has been diagnosed with urothelial carcinoma, it’s important to stay informed about the latest treatment options and research developments. One related article worth checking out is A Deep Dive into Renters Insurance: Everything You Should Consider. While this article may not directly relate to urothelial carcinoma, it’s always important to consider all aspects of your health and well-being, including protecting your belongings and financial assets. Stay informed and take care of yourself in every way possible.
FAQs
What is urothelial carcinoma?
Urothelial carcinoma, also known as transitional cell carcinoma, is a type of cancer that occurs in the urothelial cells lining the bladder, ureters, urethra, and renal pelvis.
What are the risk factors for developing urothelial carcinoma?
Risk factors for urothelial carcinoma include smoking, exposure to certain chemicals (such as those in tobacco smoke or certain industrial chemicals), chronic bladder inflammation, and certain genetic factors.
What are the symptoms of urothelial carcinoma?
Symptoms of urothelial carcinoma may include blood in the urine, frequent urination, pain during urination, and back or pelvic pain.
How is urothelial carcinoma diagnosed?
Urothelial carcinoma is typically diagnosed through a combination of medical history, physical examination, imaging tests (such as CT scans or MRIs), and urine tests to look for cancer cells.
What are the treatment options for urothelial carcinoma?
Treatment options for urothelial carcinoma may include surgery, chemotherapy, radiation therapy, immunotherapy, and targeted therapy, depending on the stage and location of the cancer.
What is the prognosis for urothelial carcinoma?
The prognosis for urothelial carcinoma depends on the stage of the cancer at the time of diagnosis, as well as the individual’s overall health and response to treatment. Early detection and treatment can improve the prognosis.